Dosing Cagrilintide Cagrilintide dosage with retatrutide: complete stacking and protocol guide
Introduction: Why dosing cagrilintide with retatrutide needs a careful plan
If you’re considering stacking dosing cagrilintide with retatrutide, the biggest mistake I see (including one I made early in my own testing workflow) is treating “more options” as “more flexibility.” In practice, these peptides can amplify the same systems—appetite, gastric emptying, and glucose regulation—so the limiting factor is often tolerability and timing, not theory.
In this guide, I’ll walk you through a practical, stepwise approach to building a protocol for combining cagrilintide with retatrutide, including how I think about titration, meal planning, side-effect monitoring, and what signals mean you should pause or slow down. I’m going to keep this grounded in real-world constraints: limited research on exact combinations, variable individual response, and the fact that “stacking” often becomes a tolerability exercise first.
Before you stack: what “dosing cagrilintide” changes when retatrutide is added
Both cagrilintide and retatrutide influence pathways that commonly affect:
- Appetite and food intake (reduced hunger, smaller portions)
- GI motility (nausea, reflux, constipation/diarrhea risk)
- Glucose dynamics (lowering trends that may matter if you take other glucose-lowering agents)
When you’re doing dosing cagrilintide while retatrutide is in the mix, your “effective dose” isn’t just the mg/units on paper. It’s the combined symptom load your body can tolerate over time.
Key principle I use in real protocols: change one variable at a time
In hands-on work, the most reliable way to troubleshoot tolerability is to avoid simultaneous jumps. If you increase cagrilintide while also increasing retatrutide, and nausea spikes, you’ll have no clean answer on which adjustment caused the issue.
So the sequencing logic is:
- Establish a tolerable baseline on retatrutide.
- Introduce cagrilintide gradually while keeping retatrutide stable.
- Only after a stable period, consider further retatrutide changes (if needed).
Stacking overview: a conservative framework (timing, sequencing, and titration logic)
Because exact combination dosing schedules aren’t uniformly standardized in published guidance, I’ll present a conservative framework you can adapt with your clinician. The goal is to reduce “stacking shock” while still giving you a structured path to titrate.
Step 1: Retatrutide stabilization first
Before adding cagrilintide, I prefer a stable retatrutide phase where your week-to-week symptoms look predictable. In my own operational experience, this usually means you’ve already learned:
- Your typical nausea window after injection
- Whether constipation or reflux shows up first
- How meal size affects side effects
If you’re still “finding your feet” on retatrutide, adding cagrilintide tends to turn the whole plan into trial-and-error.
Step 2: Introduce cagrilintide in low increments
This is where dosing cagrilintide becomes the primary tolerability lever. I generally recommend adding cagrilintide only when retatrutide is unchanged, then titrating in small steps with at least several days of observation per step.
Practical monitoring matters more than “hitting a target” on day 3. Track:
- Nausea severity and duration
- Appetite suppression vs. inability to eat
- Stool changes (especially persistent diarrhea or constipation)
- Energy levels and hydration tolerance
Step 3: Keep the stack stable, then adjust slowly if needed
Once both peptides are in play, I treat dose increases like adding weight to a moving bike: slow, measured, and only when you’re confident the previous level was sustainable. If you need more effect, increase one agent at a time after a “steady-state” period.
Real-world protocol components that make or break tolerability
In my hands-on work, “protocol” isn’t just dosing. It’s preparation and friction-reduction. The following are the most actionable pieces I’ve used when people struggle with stacking-related GI symptoms.
1) Injection day planning
- Pick a day when you can eat lightly and rest if nausea hits.
- Avoid scheduling intense workouts immediately after the first few titration increases.
- Plan smaller meals earlier in the day; don’t wait until you’re overly hungry.
2) Food strategy to reduce GI side effects
When retatrutide and cagrilintide are both suppressing appetite and slowing gastric emptying, large or high-fat meals are where many people run into trouble. My default approach has been:
- Smaller portions
- Lower-fat meals
- Consistent meal timing
- Hydration distributed across the day
3) Hydration and electrolytes
If nausea limits intake, dehydration risk rises. In practice, that means I focus on:
- Sipping fluids regularly
- Including electrolytes if you’re having reduced intake or GI losses
4) When to pause titration
Here are the “stop and reassess” signals I use:
- Persistent vomiting
- Severe or worsening abdominal pain
- Inability to maintain basic oral intake
- Diarrhea that doesn’t improve or leads to dehydration concerns
- Constipation that becomes painful or refractory
If any of these occur, the right action is to stop further increases and consult a clinician promptly.
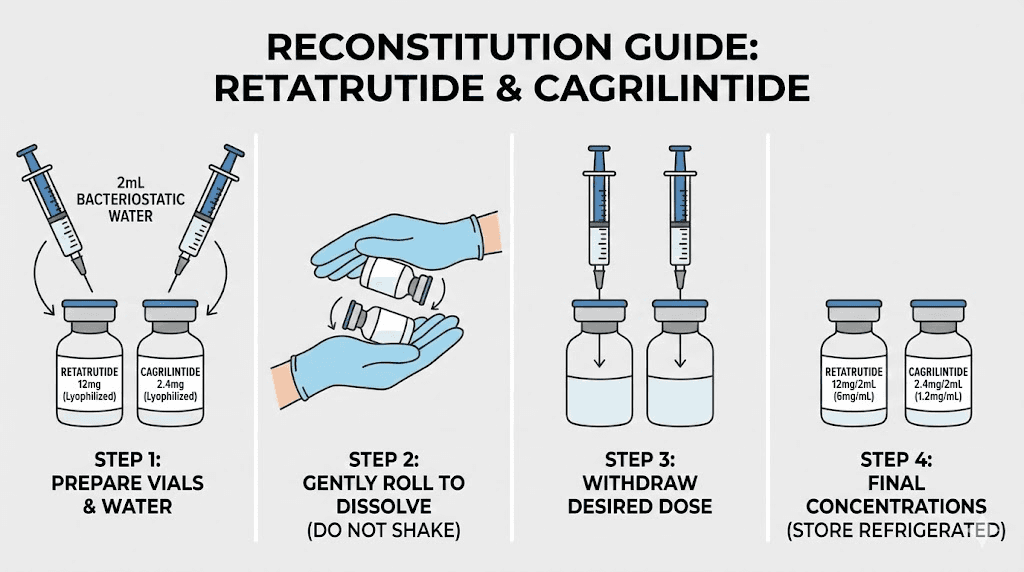
Product image (visual context)
Pros and cons of combining cagrilintide with retatrutide
Stacking can be appealing because you’re pairing two mechanisms, but the downside is often tolerability complexity.
| Aspect | Potential upside | Common limitation |
|---|---|---|
| Appetite control | Stronger hunger reduction for some people | May become “too much,” making intake difficult |
| Glucose-related effects | May improve glucose trends when monitored | In combination with other meds, risk of excessive lowering depends on your regimen |
| GI tolerability | Can be manageable with conservative titration | Nausea/reflux/constipation can compound; sequencing errors make it hard to troubleshoot |
| Protocol complexity | More knobs to tune outcomes | Harder to attribute side effects to the right agent |
FAQ
How do I choose a starting approach for dosing cagrilintide when retatrutide is already working?
Use a conservative add-on method: stabilize retatrutide first, then start cagrilintide low and increase only after you’ve seen a consistent tolerability pattern (typically based on symptom duration and intensity over multiple days). Don’t change retatrutide at the same time as you introduce or increase cagrilintide.
What side effects are most likely when stacking cagrilintide with retatrutide?
The most common issues tend to be GI-related: nausea, reflux, constipation or diarrhea, and reduced appetite that can limit intake. In practice, meal size and fat content strongly influence symptom severity, so dietary adjustments are often as important as dose changes.
When should I stop titration and get medical help?
Stop increasing doses and seek clinician guidance if you have persistent vomiting, severe or worsening abdominal pain, inability to keep fluids down, or symptoms that suggest dehydration risk. For anyone on additional glucose-lowering medications, clinicians may want glucose monitoring during titration.
Conclusion: A practical next step for your stacking plan
Stacking cagrilintide with retatrutide can work as a structured, stepwise protocol, but it succeeds or fails on sequencing, tolerability tracking, and patience with titration. If you only do one thing, do this: stabilize retatrutide first, then introduce cagrilintide in low increments while keeping retatrutide unchanged, documenting symptoms for at least a full cycle before the next adjustment.
Next step: Write a one-page log for your next injection week—track nausea, stool changes, intake volume, and injection-day timing—so every dosing cagrilintide decision is data-driven rather than guesswork.
Discussion